The Perineum
The perineum is the diamond-shaped region of the pelvic outlet below the pelvic diaphragm — the shared operative field of every procedure that crosses between the lower abdomen and the vagina, anus, urethra, or perineal body. For the reconstructive urologist and urogynecologist it is the most operationally important anatomic region of the pelvic floor: the plane of bulbar urethroplasty, radical perineal prostatectomy, AUS placement, perineorrhaphy and OASIS repair, pelvic-floor reconstruction, Fournier's debridement, vaginal / vulvar reconstruction, perineal-hernia repair, and the dissection route of essentially all posterior-approach pelvic procedures. This article focuses on surgical anatomy (boundaries, fascial pouches, neurovascular geometry), the sex-specific differences that drive male vs female reconstructive technique, and the physiology of continence, sexual function, defecation, and parturition only to the depth needed at the table.
See also The Vulva, Male Urethra, Female Urethra, The Vagina, and Pelvic Neuroanatomy.
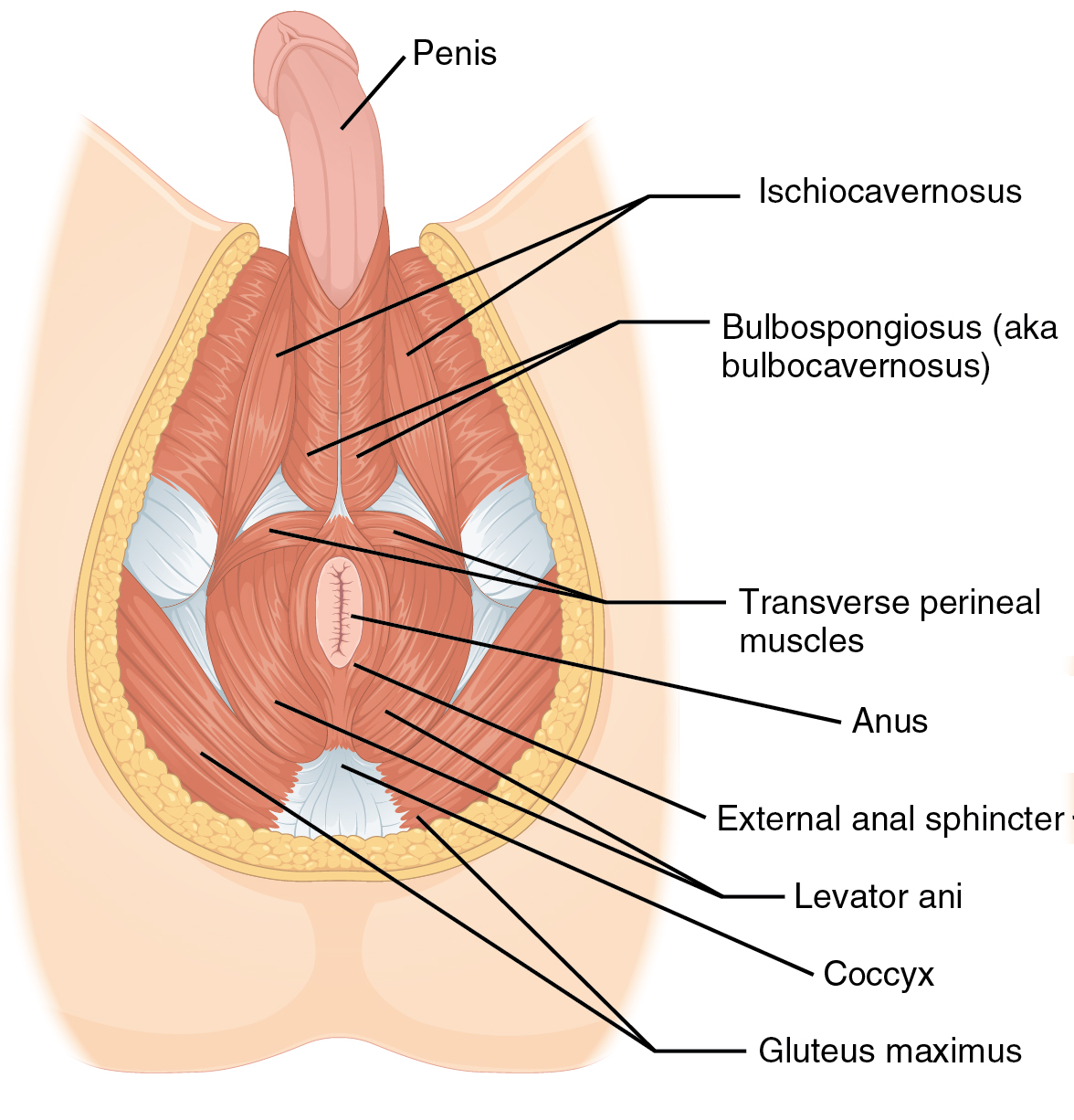
OpenStax Anatomy & Physiology — Muscles of the male perineum. (CC BY 4.0)
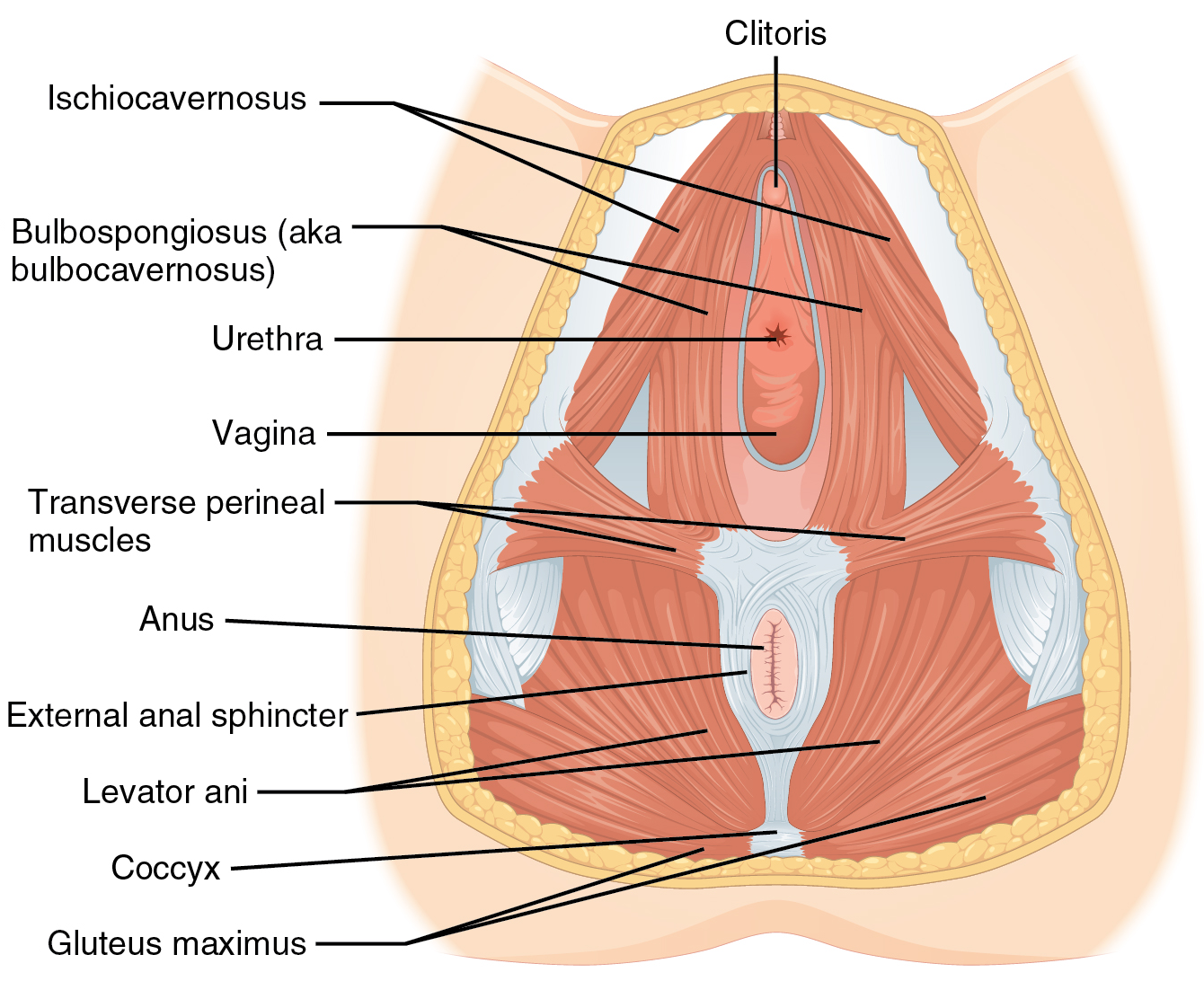
OpenStax Anatomy & Physiology — Muscles of the female perineum. (CC BY 4.0)
Boundaries and the Diamond
The perineum is bounded by four bony / ligamentous landmarks and is divided by a transverse line between the ischial tuberosities into two triangles:
| Triangle | Anterior boundary | Posterior boundary | Lateral boundary | Contents |
|---|---|---|---|---|
| Urogenital (UG) | Pubic symphysis + inferior pubic rami | Interischial line | Ischiopubic rami | Urethra, perineal membrane; vagina in women; root of penis / clitoris; Bartholin / Cowper's glands |
| Anal | Interischial line | Coccyx + sacrotuberous ligaments | Ischial tuberosities | Anal canal, external anal sphincter, ischiorectal fossae, pudendal canal |
The ischial tuberosities, pubic symphysis, and coccyx together form the four corners of the diamond. Orientation is best appreciated on the patient in lithotomy: the UG triangle is anterior (toward the surgeon); the anal triangle is posterior.
Layered Architecture — Skin to Pelvic Floor
The UG triangle has five anatomic layers, all clinically named:

Coronal slice through the urogenital triangle, between the ischiopubic rami. Two fascial pouches — superficial (bulb, crura, and their bulbospongiosus/ischiocavernosus muscles) and deep (the rhabdosphincter around the membranous urethra) — are separated by the perineal membrane, the hinge of perineal surgery and the transcorporal-AUS landmark. Colles' fascia is the roof of the superficial pouch and the plane along which Fournier's gangrene tracks. Each layer is a distinct surgical plane (blue). (Original WARWIKI schematic)
| Layer | Contents / note | Operative relevance |
|---|---|---|
| Skin | Hair-bearing; rugated over scrotum / labia majora | Plane of closure in perineorrhaphy and primary-intention perineal repair |
| Subcutaneous fat | Absent over scrotum / labia where dartos substitutes | Site of Fournier's fascial spread |
| Colles' (superficial perineal) fascia | Membranous layer; continuous anteriorly with dartos of scrotum / labia majora and with Scarpa's fascia of the abdominal wall. Fused laterally to the ischiopubic rami and posteriorly to the perineal membrane | The fascial ceiling of the superficial perineal pouch; the plane of Fournier's gangrene spread |
| Superficial perineal pouch | See contents below | The plane of bulbar urethroplasty, AUS placement, penile / clitoral root surgery |
| Perineal membrane | Two-region structure: a dorsal portion of bilateral transverse fibrous sheets attaching the lateral vaginal wall / perineal body to the ischiopubic ramus, and a ventral portion of solid tissue intimately associated with the compressor urethrae and urethrovaginal sphincter[2][3][5] | The roof of the superficial pouch and floor of the deep pouch; structural anchor of the female striated urogenital sphincter complex and of the male rhabdosphincter; landmark for AUS transcorporal placement |
| Deep perineal pouch | Rhabdosphincter (M) / striated urogenital sphincter complex (F) / Cowper's glands (M). Recent histologic work shows the "deep transverse perineal muscle" is predominantly smooth muscle continuous with rectal and vaginal walls, not a discrete striated band as classically taught[4][5][9] | The plane of pelvic-fracture urethroplasty, membranous urethral dissection, and transcorporal AUS cuff placement |
| Pelvic floor (levator ani + fascia) | Above the deep pouch | The interface with intrapelvic surgery |
Superficial perineal pouch — contents
| Men | Women |
|---|---|
| Root of the penis — bulb of corpus spongiosum (midline) + paired crura of corpora cavernosa attached to ischiopubic rami | Vestibular bulbs (paired) flanking the vagina + paired clitoral crura attached to ischiopubic rami |
| Bulbospongiosus over the bulb | Bulbospongiosus / bulbocavernosus flanking introitus |
| Ischiocavernosus over the crura | Ischiocavernosus over the clitoral crura |
| Superficial transverse perinei | Superficial transverse perinei |
| — | Bartholin (greater vestibular) glands |
| Perineal branches of the pudendal nerve and internal pudendal artery | Same |
Deep perineal pouch — contents
| Men | Women |
|---|---|
| Membranous urethra + rhabdosphincter (external urethral sphincter) — anterolateral omega-shaped loop | Urethra with the striated urogenital sphincter complex — rhabdosphincter + compressor urethrae + urethrovaginal sphincter; U-shaped anteriorly |
| Deep transverse perineal muscle | Deep transverse perineal muscle |
| Bulbourethral (Cowper's) glands | — (homologues are Bartholin's in the superficial pouch) |
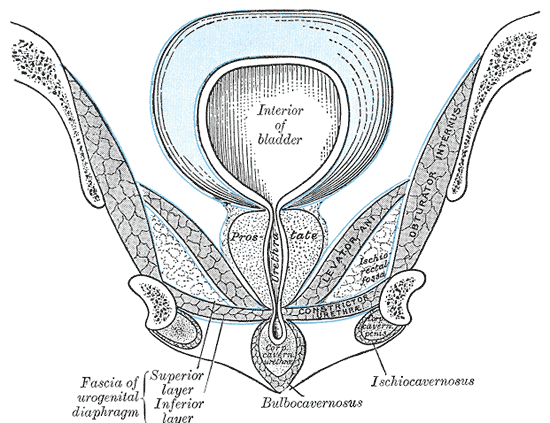
Coronal section through the pelvis and perineum. The levator ani forms the muscular pelvic floor; below it the ischiocavernosus and bulbocavernosus muscles and the urogenital diaphragm invest the urethra and erectile bodies, flanked by the fat-filled ischiorectal (ischioanal) fossae. (Public domain, Gray's Anatomy)
The Perineal Body — The Structural Anchor
The perineal body is a pyramidal fibromuscular convergence zone ~20–40 mm craniocaudally, positioned ~1–2 cm anterior to the anus in the midline between the UG and anal triangles.[12][13] It receives the insertions of:
- Bulbospongiosus / bulbocavernosus
- Superficial transverse perinei
- Deep transverse perinei
- External anal sphincter (subcutaneous and superficial parts)
- Puborectalis (superiorly)
- Posterior vaginal wall fibromuscularis (in women)
- Perineal membrane
Contemporary anatomic studies describe the perineal body as a three-layer criss-crossing scaffold rather than a simple insertion point:[13]
- Superficial layer — external-anal-sphincter fleshy fibers continuous across the midline with bulbospongiosus / bulbocavernosus.
- Middle layer — tendinous extension of the superficial transverse perinei in a criss-cross pattern.
- Deep layer — tendinous fibers of the deep transverse perinei decussating with the contralateral muscle.
Rather than terminating at the perineal body, muscle fibers often pass uninterrupted from one side to the other in a "digastric" / figure-8 pattern. Diffusion-tensor imaging has confirmed direct continuity between bulbospongiosus and the superficial external anal sphincter across the midline in >90% of specimens — evidence for shared function between the urogenital and anal triangles.[6][7]
The Perineal Complex Triad and urogenital hiatus closure. DeLancey has proposed that levator ani + perineal membrane + perineal body together form a perineal complex triad whose coordinated function closes the urogenital hiatus. Levator contraction pulls the medial perineal membrane cranioventrally, narrowing the AP diameter of the hiatus. Loss of perineal-body integrity (obstetric, surgical, or degenerative) disrupts the left–right connection of the perineal membrane, producing levator diastasis, widened genital hiatus, and downward rotation of the perineal membrane — the anatomic substrate of the posterior-compartment prolapse, rectocele, and perineal deficiency that perineorrhaphy aims to correct.[3][10]
Why the perineal body is central to reconstructive surgery. The perineal body is the structural anchor of the posterior vaginal wall and of the external anal sphincter. In women it is wider (~20–40 mm), in men narrower (~10–15 mm). Obstetric tears (2nd-, 3rd-, 4th-degree), chronic straining, and prior surgical disruption leave a thinned, gaping perineum with a deficient backstop — the anatomic substrate of rectocele, posterior compartment prolapse, fecal incontinence, and a wide genital hiatus. Reconstructing it (perineorrhaphy) is the posterior-compartment counterpart of apical suspension for anterior / apical defects.
The Anal Triangle
| Structure | Dimensions / features | Function |
|---|---|---|
| Internal anal sphincter (IAS) | ~0.3–0.5 cm thick; thickened circular smooth muscle of the rectum[15] | Under autonomic control; provides 55–80% of resting anal tone;[14][16] IAS injury → passive incontinence (unconscious leakage) |
| External anal sphincter (EAS) | ~0.6–1.0 cm thick; three-layer striated ring (subcutaneous / superficial / deep)[15]; predominantly slow-twitch, fatigue-resistant fibers | Under pudendal S2–S4 control; provides 20–30% of resting tone; voluntary contraction roughly doubles anal-canal pressure;[14][16] EAS injury → urge incontinence |
| Puborectalis | Levator-ani sling drawing anorectum anteriorly | Maintains the anorectal angle — ~90° at rest, ~70° with squeeze, ~110–130° during defecation[15] |
| Ischiorectal (ischioanal) fossa | Fat-filled paired spaces lateral to the anal canal; bounded by obturator internus laterally, levator ani superomedially, and the anal canal medially | Communicates posteriorly via a deep postanal space — the anatomic path of horseshoe abscesses |
| Pudendal (Alcock's) canal | Fascial tunnel on the medial surface of obturator internus | Carries the pudendal nerve and internal pudendal vessels |
| Anococcygeal body (ligament) | Fibromuscular raphe between anal canal and coccyx | Receives fibers of levator ani and EAS |
The entire sphincter complex extends ~4 cm up the anal canal, with the EAS overlapping the distal IAS by ~1–2 cm.
EAS subdivisions have independent innervation
A surgically useful fact: the three portions of the EAS have separate motor supplies — the subcutaneous EAS is innervated by the inferior rectal nerve (which emerges as a branch of S3–S4 distinct from the pudendal nerve in ~89% of specimens), the superficial EAS by the perineal nerve (continuous with bulbospongiosus), and the deep EAS by the nerve to levator ani.[6] This explains the variable patterns of incontinence after focal neural or sphincter injury.
Vascular Supply
Arterial
The dominant supply is the internal pudendal artery (anterior division of the internal iliac). It exits the pelvis through the greater sciatic foramen, wraps around the ischial spine, re-enters the perineum through the lesser sciatic foramen, and runs through Alcock's canal on the medial obturator internus. It terminates in four pairs of branches:
| Branch | Territory |
|---|---|
| Inferior rectal artery | Anal canal, EAS, perianal skin |
| Perineal artery (→ posterior scrotal / labial, transverse perineal) | Superficial pouch, scrotum / labia, perineal body |
| Artery of the bulb of the penis (M) / vestibular bulb (F) | Bulb of spongiosum / vestibular bulb |
| Urethral artery and dorsal / deep artery of the penis (M) / clitoris (F) | Urethral corpus spongiosum; dorsal NVB; cavernosal / corporeal engorgement |
The external pudendal arteries (from the femoral) supply anterior scrotum / anterior labia majora and mons skin — the axial vessels of the Martius labial fat-pad flap.
Venous and lymphatic
Venous drainage parallels the arteries. The deep dorsal vein of the penis / clitoris drains into the prostatic (Santorini's) plexus; superficial veins drain to the external pudendal / saphenous system.
Lymphatic drainage is split:
- Perineal skin and superficial structures → superficial inguinal nodes
- Deeper structures (bulb, urethra, deep pouch) → internal iliac basins
- This split drives the inguinal-LND template in vulvar / penile SCC and the pelvic-LND template in posterior urethral cancer.
Innervation — The Pudendal Nerve Dominates
Pudendal nerve (S2–S4)
The principal nerve of the perineum. After traversing Alcock's canal it gives three terminal branches:
| Branch | Territory / function |
|---|---|
| Inferior rectal nerve | EAS motor; perianal sensation |
| Perineal nerve — deep | Bulbospongiosus, ischiocavernosus, transverse perinei, external urethral rhabdosphincter (via Onuf's nucleus) |
| Perineal nerve — superficial (posterior scrotal / labial) | Posterior scrotum / labia majora sensation |
| Dorsal nerve of the penis / clitoris | Dominant sensory input to the glans |
Additional peripheral contributions:
- Ilioinguinal + genital branch of genitofemoral (L1–L2) — anterior scrotum / labia majora / mons
- Posterior femoral cutaneous — perineal branch — lateral perineum / upper medial thigh
- Autonomic fibers from the inferior hypogastric plexus — erectile tissue, glands, and pelvic viscera; cavernous / clitoral nerves ride with the lateral NVB and with the posterior route (see The Penis)
Onuf's nucleus
A discrete S2–S4 motor-neuron pool in the ventral horn of the spinal cord that innervates the striated external urethral and external anal sphincters. Uniquely spared in amyotrophic lateral sclerosis (ALS), which is why continence typically persists even in advanced disease — a useful clinical pearl for differential diagnosis of neurogenic continence disorders.
Dorsal penile / clitoral nerve — the sensory-critical branch
Runs on the dorsal surface of the organ adherent to the periosteum of the ischiopubic ramus (see The Penis / The Vulva). The 12 o'clock midline is relatively nerve-poor in men (the anatomic basis of the dorsal penile nerve block at the 10- and 2-o'clock positions). Injury during vestibulectomy, clitoral or penile reconstruction, or pelvic-fracture urethroplasty is the commonest cause of iatrogenic sensory loss to the organ.
Physiology
The perineum is a shared functional platform for four overlapping functions. Preservation or reconstruction of any one of them often requires trading off against another.
Continence
- External urethral sphincter (voluntary, pudendal) provides phasic closure on cough and Valsalva and a tonic contribution to resting urethral pressure. The guarding reflex recruits the sphincter reflexively before abdominal pressure rises.
- Anal continence depends on a layered mechanism:[14][15][16][18]
- Mechanical — IAS tone (bulk of resting pressure), EAS squeeze (voluntary reinforcement), puborectalis-generated anorectal angle (flap-valve), and the sealing effect of anal mucosal folds and vascular cushions.
- Sensory — pelvic-floor stretch receptors detect rectal distension; anal-transition-zone receptors discriminate gas, liquid, and solid ("rectoanal sampling").
- Reflex — the rectoanal inhibitory reflex relaxes the IAS on rectal distension, allowing sampling. Involuntary EAS / puborectalis / sphincter-of-O'Beirne contractions, together with retrograde propagating sigmoid and rectal motor patterns, prevent continuous anal outflow between defecations.[18]
- Pelvic-floor / perineal backstop — the perineal body, perineal membrane, and levator-ani complex form the posterior hammock against which the bladder neck / urethra (and, in women, anterior vaginal wall) are compressed by abdominal pressure. Loss of this backstop is the structural cause of much of female stress urinary incontinence (see The Vagina).
Sexual function
- Ischiocavernosus — reflexively contracts on sexual stimulation, compressing the crura of the penis / clitoris and trapping blood in the corpora; generates suprasystolic intracavernous pressures required for rigid erection and clitoral engorgement.[8]
- Bulbospongiosus / bulbocavernosus — in men, contracts to expel semen and urine through the urethra and maintains intraspongiosal pressure; in women, contributes to introital narrowing, clitoral engorgement via vestibular-bulb compression, and the rhythmic contractions of orgasm.
- Erectile tissue of the clitoris, vestibular bulbs, corpora cavernosa, and corpus spongiosum — autonomic-driven engorgement during arousal.
- Sensory dominance of the glans — via the dorsal nerve of the penis / clitoris; the highest nerve density of the perineum.
- Three-part reflex control: erection is parasympathetic-dominant (S2–S4, NO-mediated vasodilation); emission is sympathetic-dominant (T10–L2, contraction of vas deferens, seminal vesicles, and prostate); ejaculation is somatic-dominant (S2–S4 via pudendal) with rhythmic bulbospongiosus and ischiocavernosus contractions. A spinal generator of ejaculation composed of premotor interneurons at L3–L5 coordinates the response — integrity of these segments is required for antegrade ejaculation, which is why suprasacral spinal-cord injury above L3 typically abolishes it.[19][20]
Defecation
- Voluntary relaxation of puborectalis opens the anorectal angle.
- Voluntary relaxation of EAS combined with reflex IAS relaxation on rectal distension permits evacuation.
- Perineal-body support of the posterior vaginal wall in women prevents rectocele bulge during straining; deficit causes paradoxical anterior bulging rather than evacuation.
Childbirth
- The perineum stretches markedly during the second stage of labor.
- The perineal body is the most common site of obstetric laceration.[1]
- Episiotomy, when indicated, is typically mediolateral rather than midline (lower risk of 3rd/4th-degree extension).[1]
- Obstetric anal sphincter injuries (OASIS) — 3rd-degree (EAS involvement) and 4th-degree (rectal mucosa) tears — disrupt the perineal-body convergence and are the reconstructive target of primary repair; delayed / symptomatic defects may be addressed with overlapping sphincteroplasty, biofeedback, or sacral neuromodulation.[16][21]
- Levator ani avulsion is an often unrecognised component of birth injury — MRI identifies visible levator defects in approximately 20% of primiparous women,[11] correlating with downstream pelvic-organ-prolapse risk.
Vascular Anatomy of Perineal Perforator Flaps
Beyond the internal and external pudendal supply described above, four relatively constant perforating arteries have been mapped in the perineum and are the vascular basis of perforator-flap reconstruction:[17]
- Inguinal perforating branch of the superficial external pudendal artery
- Perineal perforating branch of the superficial external pudendal artery
- Perforating branch of the anterior cutaneous branch of the obturator artery
- Perforating branch of the lateral branch of the posterior scrotal / labial artery
These form upper, middle, and lower anastomoses in the deep fascia above the adductor compartment — the anatomic substrate for the pudendal-thigh (Singapore), internal pudendal artery perforator (IPAP), and anterior obturator artery perforator flaps used in vaginal, vulvar, and perineal reconstruction.
Sex Differences for the Reconstructive Surgeon
| Feature | Men | Women |
|---|---|---|
| UG-triangle contents | Single pass-through (urethra); bulb + crura of penis | Double pass-through (urethra + vagina); vestibular bulbs + clitoral crura |
| Perineal body | Narrower (~10–15 mm); less structural role | Wider (~20–40 mm); central reconstructive target for posterior compartment and EAS support |
| Sphincter geometry in deep pouch | Rhabdosphincter as anterolateral omega-loop around membranous urethra | Striated sphincter complex U-shaped in distal 2/3 of urethra, embedded in perineal membrane |
| Homologue glands | Cowper's (bulbourethral) — in the deep pouch | Bartholin (greater vestibular) — in the superficial pouch |
| Scrotum / labia majora | Scrotum + dartos | Labia majora + dartos; Martius flap territory |
| Clitoris vs penis | Same embryologic plan — glans, body, paired crura; dorsal nerve is the sensory-critical structure in both | |
| Operative targets | Bulbar urethroplasty, AUS, radical perineal prostatectomy, PFUI repair | Perineorrhaphy, OASIS repair, vestibulectomy, Martius flap harvest, vaginal reconstruction |
Clinical Correlations for the Reconstructive Surgeon
- Bulbar urethroplasty. The bulbar urethra sits in the superficial perineal pouch invested by bulbospongiosus. Perineal incision → midline split of bulbospongiosus → mobilise the corpus spongiosum → perform anastomotic or augmentation repair. The central perineal tendon (perineal body) is preserved to avoid postoperative anterior ejaculatory dysfunction and perineal weakness.
- Artificial urinary sphincter (AUS) cuff placement. Perineal approach to the bulbar urethra; cuff placed around the corpus spongiosum distal to the crura. Transcorporal cuff placement (through the tunica of the corpora cavernosa) reinforces a compromised spongiosum in reoperative or radiation cases.
- Radical perineal prostatectomy and perineal approach to the prostate. Curved incision anterior to the anus, through the central tendon, between ischiocavernosus muscles, exposing the prostate posterior to the bulb. Useful historically and in selected patients where abdominal access is contraindicated.
- Pelvic-fracture urethral injury (PFUI) repair. Perineal approach with crural separation, infrapubic resection, and anastomotic urethroplasty; deep-pouch dissection required for proximal exposure. Supracrural or transpubic extensions for long or complex defects.
- Perineorrhaphy and OASIS repair. Reconstruct the perineal body's convergence of bulbospongiosus and transverse perinei. In OASIS: reconstitute IAS (when disrupted), EAS (end-to-end or overlapping sphincteroplasty), and the perineal-body muscular convergence; close overlying vaginal mucosa and perineal skin.
- Vestibulectomy for vulvodynia. Excision of painful vestibule with vaginal advancement flap — the neuroproliferative vestibulodynia operation. See The Vulva.
- Martius labial fat-pad flap. The perineum's workhorse interposition flap: VVF, RVF, UVF, urethral diverticulectomy, complex perineal wounds. Harvested through a vertical labia-majora incision; pedicle choice (superior external pudendal vs inferior internal pudendal) dictates reach. See The Vulva.
- Gracilis muscle flap. Reliable regional flap for large perineal defects (rectovaginal / rectourethral fistulae, perineal hernia after APR, vulvar reconstruction). Pedicled on the medial circumflex femoral artery.
- Pudendal-thigh (Singapore) fasciocutaneous flap. Axial flap from the groin crease supplied by branches of the internal pudendal artery; used for vaginal, vulvar, and perineal reconstruction.
- Fournier's gangrene. Necrotizing fasciitis of the dartos / Colles' / Scarpa's plane; testes and cord usually spared. Emergency wide debridement, broad-spectrum antibiotics, diversion as needed, delayed reconstruction.
- Perineal hernia. Post-APR / post-exenteration defect through the levator and perineal floor; reconstructed with biologic mesh + muscle flap (gracilis, VRAM).
- Ischiorectal fossa abscess / horseshoe abscess. Drained through the anal triangle; attention to the deep postanal space where horseshoe abscesses bridge. Unrecognised horseshoe extensions produce recurrent abscess / complex fistula.
- Pudendal neuralgia and Alcock's canal entrapment. Burning perineal / clitoral / scrotal pain worse sitting, relieved standing. Nantes criteria drive diagnosis. Pudendal nerve block is therapeutic and diagnostic; refractory cases → surgical decompression of Alcock's canal.
- Sacrospinous ligament fixation (SSLF). Vaginal-vault suspension to the sacrospinous ligament near the ischial spine — directly adjacent to the pudendal NVB in Alcock's canal. Injury produces gluteal / perineal pain and pudendal neuropathy.
- Radical vulvectomy and perineal reconstruction. After wide local excision or radical vulvectomy ± inguinal LND. Reconstruction ladder: primary closure → local V-Y or rhomboid flaps → Singapore (pudendal-thigh) flap → gracilis or VRAM myocutaneous flap for large defects.
- Cauda equina and S2–S4 lesions. Produce perineal ("saddle") anesthesia, loss of pudendal function with EAS and external urethral sphincter denervation — a neurogenic-continence phenotype unique to this level.
- Male sling procedures. Transobturator male slings for mild-to-moderate post-prostatectomy SUI anchor at the pubic rami and compress the bulbar urethra; anatomic knowledge of the perineal pouch and the dorsal NVB avoids sensory injury.
- Pelvic radiation sequelae. Chronic perineal skin changes, impaired flap viability, fistula formation — non-irradiated interposition flaps (Martius, gracilis, omental) are mandatory for repair of post-radiation fistulae.
- Gender-affirming surgery (perineal component). Phalloplasty / metoidioplasty use perineal tissue for urethral lengthening; vaginoplasty creates the neovaginal cavity in the plane between urethra/prostate (anterior) and rectum (posterior), with the perineal body preserved to support the introitus.
References
1. Committee on Practice Bulletins-Obstetrics. "ACOG Practice Bulletin No. 198: Prevention and Management of Obstetric Lacerations at Vaginal Delivery." Obstet Gynecol. 2018;132(3):e87–e102. doi:10.1097/AOG.0000000000002841
2. Stein TA, DeLancey JO. "Structure of the Perineal Membrane in Females: Gross and Microscopic Anatomy." Obstet Gynecol. 2008;111(3):686–693. doi:10.1097/AOG.0b013e318163a9a5
3. DeLancey JO, Pipitone F, Masteling M, et al. "Functional Anatomy of Urogenital Hiatus Closure: The Perineal Complex Triad Hypothesis." Int Urogynecol J. 2024;35(2):441–449. doi:10.1007/s00192-023-05708-w
4. Muro S, Chang L, Tharnmanularp S, et al. "Presence of Smooth Muscle Continuous With the Rectal and Vaginal Walls in the Deep Perineal Space Prompts Reconsideration of the Deep Transverse Perineal Muscle." Sci Rep. 2025;15(1):23730. doi:10.1038/s41598-025-09585-9
5. Kampelmann M, Grindley C, Mühlfeld C, Schmiedl A. "Macroscopical and Histological Characterization of the Perineal Membrane and Deep Perineal Pouch." J Anat. 2026;248(5):755–765. doi:10.1111/joa.70057
6. Plochocki JH, Rodriguez-Sosa JR, Adrian B, Ruiz SA, Hall MI. "A Functional and Clinical Reinterpretation of Human Perineal Neuromuscular Anatomy: Application to Sexual Function and Continence." Clin Anat. 2016;29(8):1053–1058. doi:10.1002/ca.22774
7. Zifan A, Reisert M, Sinha S, et al. "Connectivity of the Superficial Muscles of the Human Perineum: A Diffusion Tensor Imaging-Based Global Tractography Study." Sci Rep. 2018;8(1):17867. doi:10.1038/s41598-018-36099-4
8. Schmidt MH, Schmidt HS. "The Ischiocavernosus and Bulbospongiosus Muscles in Mammalian Penile Rigidity." Sleep. 1993;16(2):171–183. doi:10.1093/sleep/16.2.171
9. Hinata N, Murakami G. "The Urethral Rhabdosphincter, Levator Ani Muscle, and Perineal Membrane: A Review." Biomed Res Int. 2014;2014:906921. doi:10.1155/2014/906921
10. Jelovsek JE, Maher C, Barber MD. "Pelvic Organ Prolapse." Lancet. 2007;369(9566):1027–1038. doi:10.1016/S0140-6736(07)60462-0
11. Singh K, Reid WM, Berger LA. "Magnetic Resonance Imaging of Normal Levator Ani Anatomy and Function." Obstet Gynecol. 2002;99(3):433–438. doi:10.1016/s0029-7844(01)01743-4
12. Vukasović I, Kalafatić D, Banović M, Banović V. "Ultrasound Assessment of the Perineal Body: A Scoping Review." Eur J Obstet Gynecol Reprod Biol. 2025;318:114904. doi:10.1016/j.ejogrb.2025.114904
13. Shafik A, Sibai OE, Shafik AA, Shafik IA. "A Novel Concept for the Surgical Anatomy of the Perineal Body." Dis Colon Rectum. 2007;50(12):2120–2125. doi:10.1007/s10350-007-9064-8
14. Madoff RD, Williams JG, Caushaj PF. "Fecal Incontinence." N Engl J Med. 1992;326(15):1002–1007. doi:10.1056/NEJM199204093261507
15. Rao SS; American College of Gastroenterology Practice Parameters Committee. "Diagnosis and Management of Fecal Incontinence." Am J Gastroenterol. 2004;99(8):1585–1604. doi:10.1111/j.1572-0241.2004.40105.x
16. Madoff RD, Parker SC, Varma MG, Lowry AC. "Faecal Incontinence in Adults." Lancet. 2004;364(9434):621–632. doi:10.1016/S0140-6736(04)16856-6
17. Jin B, Hasi W, Yang C, Song J. "A Microdissection Study of Perforating Vessels in the Perineum: Implication in Designing Perforator Flaps." Ann Plast Surg. 2009;63(6):665–669. doi:10.1097/SAP.0b013e3181999de3
18. Trzpis M, Sun G, Chen JH, Huizinga JD, Broens P. "Novel Insights Into Physiological Mechanisms Underlying Fecal Continence." Am J Physiol Gastrointest Liver Physiol. 2023;324(1):G1–G9. doi:10.1152/ajpgi.00313.2021
19. Courtois F, Carrier S, Charvier K, Guertin PA, Journel NM. "The Control of Male Sexual Responses." Curr Pharm Des. 2013;19(24):4341–4356. doi:10.2174/13816128113199990333
20. Hentzen C, Musco S, Amarenco G, Del Popolo G, Panicker JN. "Approach and Management to Patients With Neurological Disorders Reporting Sexual Dysfunction." Lancet Neurol. 2022;21(6):551–562. doi:10.1016/S1474-4422(22)00036-9
21. Rao SS. "Pathophysiology of Adult Fecal Incontinence." Gastroenterology. 2004;126(1 Suppl 1):S14–S22. doi:10.1053/j.gastro.2003.10.013